Your instinct is right. We make it defensible.
Decision infrastructure for hospitals. Not another AI tool — the system that replaces the $500K consultant and stays.
This isn't a tool you log into. It's a strategic engagement that produces permanent infrastructure.
As Featured In
Selected through WEDC's Accelerate Wisconsin initiative as one of five startups for gBETA Madison.
Every Hospital Makes Million-Dollar Decisions With No System
of hospital executives rank financial pressure as their #1 threat. Yet when a CEO decides to close a service line, restructure staffing, or allocate capital — there's no structured process. No documented alternatives. No record of why.
Hospitals spend $30 billion on data systems — EHR, dashboards, analytics. Zero on decision infrastructure.
The spreadsheet says save $800K. Eighteen months later, the cascade costs $4.5M. Same data. Opposite answer.
Entity Flow closes that gap.
What Entity Flow Is — and Isn't
Another AI dashboard
CIOs review hundreds of them.
Another health IT vendor
No EHR integration. No IT overhead.
A consulting engagement
Consultants leave a PDF and walk away.
A ChatGPT wrapper
Generic AI gives you a paragraph.
The system that captures WHY
Board-ready. Audit-proof. Permanent.
A service, not a tool
We sit with your CEO. Then the system learns.
McKinsey that stays
Same quality analysis. Fraction of the cost. Forever.
Built on a decade of research
14M Medicare claims. Harvard PhD. 5 deployments.
We Don't Install Software. We Sit With Your CEO.
Conversation
We meet with your leadership team. No demo. No setup. We talk about the hardest decision on your plate.
Context
We bring in what your spreadsheet can’t — community data, policy changes, workforce trends, historical patterns.
Analysis
Four options. Costs in dollars. Trade-offs mapped. Assumptions you can adjust. Updated in real time.
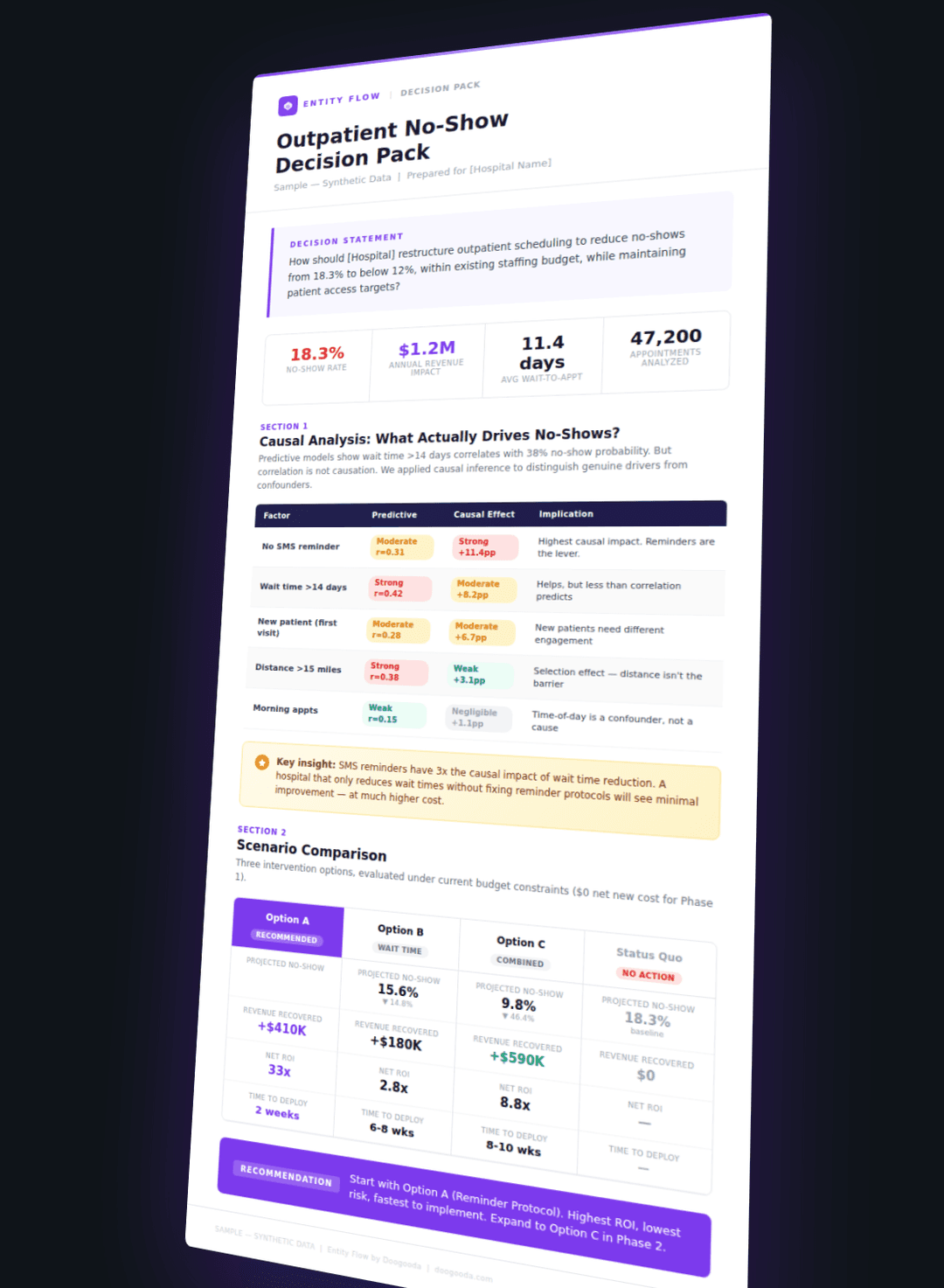
Decision Pack
Board-ready. Audit-proof. With reversal conditions — the specific trigger that says ‘revisit this decision.’ Your reasoning. Permanent.
Conversation
We meet with your leadership team. No demo. No setup. We talk about the hardest decision on your plate.
Context
We bring in what your spreadsheet can’t — community data, policy changes, workforce trends, historical patterns.
Analysis
Four options. Costs in dollars. Trade-offs mapped. Assumptions you can adjust. Updated in real time.
Decision Pack
Board-ready. Audit-proof. With reversal conditions — the specific trigger that says ‘revisit this decision.’ Your reasoning. Permanent.
Every engagement makes the system smarter. The first Decision Pack takes a week. The tenth takes a day. That's the platform building itself.
The Math Is Simple
McKinsey project
$500,000
Leaves a PDF
Data analyst hire
$85,000/yr
If you can find one
Entity Flow
$42,000/yr
Permanent. Cumulative.
One avoided bad decision
$500,000 – $4,500,000
ROI
12x – 107x
Half the cost of a data analyst. A fraction of McKinsey. Hundred-x ROI on one avoided mistake.
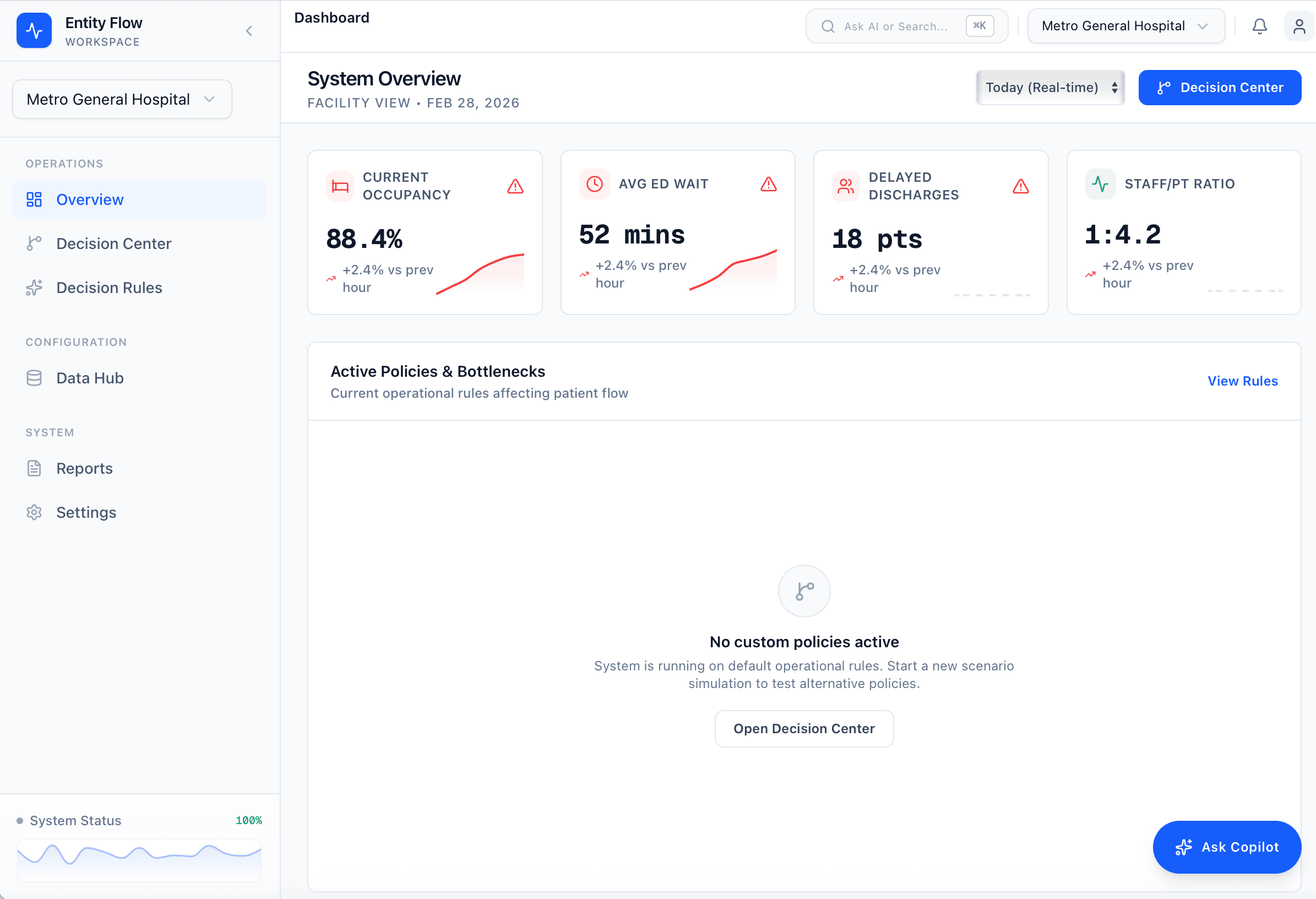
What we see before the first meeting.
Built from public data alone — no internal files, no EHR access, no NDA. Hover nodes to explore relationships. Yellow edges reveal decision leverage points.
WHERE DECISIONS HIDE
Each node is a public data point. Most hospitals already track them — separately, in different departments, on different dashboards. The yellow edges are what matters: 670 open positions don't just mean “we're hiring” — they predict ED wait time pressure. A 3.6% margin doesn't just mean “tight” — it constrains every staffing decision for the next two years. Entity Flow connects these into auditable decisions, not more dashboards.
All data from publicly available sources. No internal hospital data used. · Entity Flow by Doogooda
Built Over a Decade. Deployed Across 3 Countries.
Built by people who've done this before.

Lina Song
CEO & Founder
- •Harvard PhD (Health Policy & Decision Science)
- •Trained in the program founded by Milton Weinstein (founder of cost-effectiveness analysis)
- •PhD committee: Richard Zeckhauser (decision theory), Joseph Newhouse (health economics)
- •NIH/AHRQ-funded Principal Investigator — US Medicare claims data
- •Taught machine learning at Harvard | MS Statistics (Yale) | BS Applied Math (Caltech)
- •Former faculty at UCL and Cornell
- •Clinical experience: Moorfields Eye Hospital NHS, MGH
- •AcademyHealth Best Paper Award · Published in Management Science
CTO
- •Full-stack CTO · 10+ years shipping production systems at 50M+ user scale
- •Led platform reliability and infrastructure for one of Asia's largest consumer tech companies
- •DevOps/SRE · Cloud architecture · Security & compliance · AI/ML
- •At Entity: translates complex healthcare operational data into secure, auditable, enterprise-grade decision systems
One built the decision science. The other builds the systems that run it.
Research-grade methodology. Production-grade engineering.
Questions We Get
Epic records what happened to a patient. Entity Flow captures why your hospital made an operational decision. They’re different systems solving different problems. We sit on top of Epic, not instead of it. No integration needed.
Generic AI gives you a paragraph with no audit trail. Entity Flow gives you a board-ready decision artifact — with costs, alternatives, and reversal conditions — built on a hospital decision ontology from 14M Medicare claims. The interface is simple. The engine took a decade to build.
Consultants leave a PDF and walk out the door. But the bigger problem: that analysis is static. Six months later, conditions change — Medicaid rates shift, your workforce changes, a nearby hospital closes. The McKinsey PDF doesn’t update. You’d have to hire them again. Entity Flow builds living infrastructure. Set reversal conditions, and when the world changes, the system tells you to revisit. No second engagement. No second invoice.
You probably engage them once or twice a year on your biggest decisions. What about the other 50 operational decisions? What happens when the assumptions behind last year’s McKinsey analysis change? Entity Flow gives you the same rigor — permanently. Your team can revisit, adjust assumptions, and run new scenarios without calling the consultants back.
A 25-bed hospital closing its only maternity unit is one of the most complex decisions in healthcare. Small doesn’t mean simple. Entity Flow costs $42K/year — half a data analyst. One avoided mistake pays for a decade of service.
No EHR integration. No patient data. We work with operational and financial data — the same information your CEO discusses in board meetings. No HIPAA-covered data required.
Let's Start With a Conversation
No demo. No setup. Just 30 minutes about the hardest decision on your plate. If Entity Flow can help, we'll show you how.
ceo@doogooda.com · doogooda.com · linasong.com